

Dengue Virus in NJ: Some Considerations
Dengue Virus in NJ: Some Considerations

Despite the introduction of dengue vaccines, widespread use of toxic pesticides and the release of billions of genetically-modified mosquitoes, cases of dengue are at an all-time high across North, Central and South America.
On June 25, 2024, the CDC issued a Health Alert Network (HAN) message regarding an increased risk of dengue virus (DENV) infections in the US. Dengue viruses, of which there are four known serotypes, are transmitted by infected Aedes mosquitoes, which can also potentially transmit Zika, Chikungunya, yellow fever, and West Nile virus (more on this later).
Forty-two DENV cases have been reported in New Jersey in people who contracted it while traveling.
Heightened surveillance means infection numbers will likely climb despite the fact that all NJ cases have been brought in from other places and no local transmission has been reported. Furthermore, the introduction of the WHO’s Global Arbovirus Initiative in 2022 means that public health organizations have been primed to be on the lookout for Dengue, Yellow fever, Chikungunya and Zika viruses.
This is a good time to learn more about dengue diagnosis, surveillance and the specific risks associated with existing vaccines.
Dengue Surveillance
According to the CDC:
In the setting of increased global and domestic incidence of dengue, healthcare providers should take steps including:
Have increased suspicion of dengue among people with fever who have been in areas with frequent or continuous dengue transmission within 14 days before illness onset,
Order appropriate diagnostic tests for acute DENV infection: reverse transcription polymerase chain reaction [RT-PCR] and IgM antibody tests, or non-structural protein 1 [NS1] antigen tests and IgM antibody tests,
Ensure timely reporting of dengue cases to public health authorities, and
Promote mosquito bite prevention measures among people living in or visiting areas with frequent or continuous dengue transmission.
But the CDC also says:
Serologic testing by IgG in a single specimen is not recommended for diagnosis of acute dengue in patients, as these tests may detect antibodies from dengue infections or other flavivirus infections that occurred in the past
(other flavivirus infections include Japanese encephalitis, Kyasanur Forest disease, Powassan virus, West Nile virus, Yellow fever virus, and Zika virus)
And
A negative result from a RT-PCR or NS1 test does not rule out infection.
And let’s not forget about “presumptive diagnosis”:
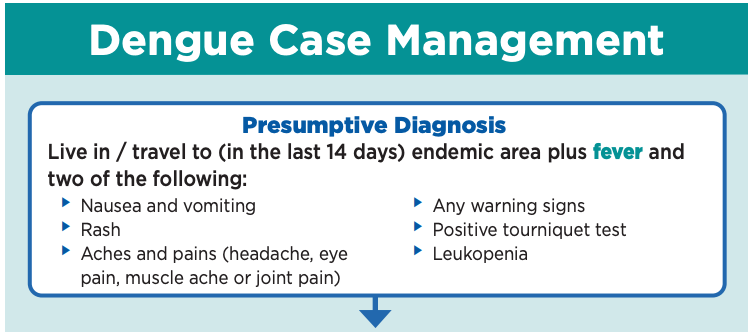
Suffice it to say, there’s a dengue virus hunt in progress. Expect the bar (and the cycle thresholds) to wobble.
And things are likely about to get interesting, because having an initial exposure to dengue makes you eligible for available dengue vaccines. This is potentially the birth of a new and ever-expanding target market.
About Dengue
Back to the NJ 101.5 article:
Those who are infected don’t get sick but some experience headache, fever and flu-like symptoms like nausea and vomiting which usually last up to a week.
This is a pretty confusing explanation, so let’s look at what the CDC has to say about DENV infection:
Approximately one in four DENV infections are symptomatic and can be mild or severe. Symptoms begin after an incubation period of 5–7 days (range 3–10 days) and present as fever accompanied by non-specific signs and symptoms such as nausea, vomiting, rash, muscle aches, joint pain, bone pain, pain behind the eyes, headache, or low white blood cell counts.
So 75% of DENV infections do NOT result in symptoms and when they do, many presentations are very similar to those of other mosquito-borne and viral illnesses.
Severe disease, with associated severe bleeding, shock or respiratory distress caused by plasma leakage, or end-organ impairment, develops in 1 in 20 people with symptomatic dengue. Infants aged ≤1 year, pregnant people, adults aged ≥65 years, and people with certain medical conditions are at increased risk of severe dengue. Although a second DENV infection (i.e., with a different DENV from the first infection) carries a higher risk of severe disease than a first, third, or fourth infection, any infection can lead to severe disease.
So, 5% of the 25% who become symptomatic can develop serious disease. Exposure to a different strain after an initial infection is linked to an increased risk of severe disease. (This is important!) Other risk factors include: hypertension, diabetes, asthma, chronic kidney disease, chronic liver disease, peptic ulcer disease or other gastritis, and receiving anticoagulation medications.
Once again, it appears that we’re looking at a disease of vulnerability.
The Checkered History of Dengue Vaccines (and other “solutions)
I’ve learned to be skeptical of public health “solutions.” This article, which I republished yesterday, helps explain why.

For example, this NEVER gets talked about…
The Zika virus is strikingly similar to the dengue virus, which has four different strains. They all belong to the Flaviviridae family. Research from the NIH’s Biomedical Research Centre suggests that, due to similarities in their genetic make-up, pre-existing dengue antibodies can amplify a Zika infection through a phenomenon called antibody-dependant enhancement (ADE). This same phenomenon explains why most people who get dengue fever have a mild first infection, but can experience severe, hemorrhagic symptoms with a second infection. Immunity from one strain of dengue does not protect someone from the other strains; instead antibody-dependent enhancement allows other strains to piggyback into the immune system undetected, leaving the body more vulnerable. This has plagued dengue vaccine efforts for decades, as vaccine antibodies can act like a silent initial infection, making way for a severe reaction if a person is exposed to a different strain in the future.
In September of 2014, vaccine developer Sanofi Pasteur also announced that it had conducted the final landmark efficacy study of its dengue vaccine candidate in dengue endemic areas in Brazil, Colombia, Mexico, Honduras and Puerto Rico,20 all significant sites of Zika outbreaks. This is particularly relevant since a York University study suggests that vaccinating against dengue could cause additional Zika outbreaks.21
Keeping this in mind, let’s review current recommendations.
The CDC’s Emergency Preparedness and Response Alert has this to say regarding dengue vaccines:
In June 2021, the Advisory Committee of Immunization Practices recommended a dengue vaccine, Dengvaxia, for children aged 9–16 years with laboratory confirmation of previous DENV infection and living in areas with frequent or continuous dengue transmission such as Puerto Rico. While the vaccine is considered safe and effective, the manufacturer (Sanofi Pasteur, Inc., Paris France) has discontinued production citing a lack of demand. Vaccine administration will continue in Puerto Rico until available doses expire in 2026. There are no vaccines recommended for travelers, adults, or persons without a previous DENV infection. (emphasis mine)
I’m guessing that this last part is largely because the VAST majority of Americans don’t have previous dengue infections, putting most of the population at risk for more serious illness associated with antibody-dependent enhancement. I’d be very curious to see how the current scare impacts that piece of the narrative. It’s probably also a good idea to track the release of genetically-modified mosquitos and the “unintended consequences” that ensue.

Back to vaccines…
“Laboratory confirmation of previous DENV infection” is now required prior to administration of Dengvaxia because of a costly lesson for children in the Philippines that never should have been necessary.
I wrote about this back in 2020.

Despite 20 years of research and multiple clinical trials, Dengvaxia caused injury and death among the very population it was designed to serve. How did this vaccine make its way past all of the gatekeepers who were put in place to ensure a “safe and effective” candidate? Why, in 2016, did a panel at the World Health Organization (WHO) go ahead and declare Dengvaxia safe and recommend it for children aged 9 and older? Was the scientific community unaware of potential risks and shortcomings? Did the deaths of children in the Philippines come as a complete surprise?
They shouldn’t have.
…Early signs of a problem with the dengue vaccine surfaced back in 2012 when researchers observed that it protected against three of the four dengue virus serotypes but failed to provide protection against the fourth—serotype 2—then the most prevalent. In July 2014, an article published in Science (entitled “Dengue vaccine trial poses public health quandary”) described the emerging dilemma:
“The first large efficacy trial of a vaccine for the tropical disease dengue has returned puzzling results. The vaccine, developed by Sanofi Pasteur, proved safe, had an overall efficacy rate of 56.5%, and reduced cases of severe disease by 88.5%. But it had limited efficacy against dengue 2, one of four dengue virus serotypes in circulation [emphasis added]…. In considering the vaccine for national immunization programs, public health officials will have to carefully weigh the benefits of reducing that burden against the yet-to-be-determined cost of the vaccine and its limited efficacy against dengue 2. The results also pose quandaries for scientists. The trial showed that a standard in vitro assay used to predict the level of immunity in vaccines correlated poorly with actual protection from disease.”
Retired dengue expert, Scott Halstead, asserted that the Dengvaxia vaccine should not be given to children who had never had a dengue infection, as it might mimic the effect of an initial infection and, therefore, make children vulnerable to a more severe presentation later. In fact, a 2011 paper had already issued a clear warning about the need to avoid antibody-dependent enhancement:
Serious disease can be seen during primary infection but is more frequent following second infection with a serotype different from that of a previous infection…. The high level of virus replication seen during both secondary infection with a heterotypic virus and during primary DENV infection in late infancy is a direct consequence of antibody-dependent enhancement of replication. This enhanced virus replication is mediated primarily by preexisting, nonneutralizing, or subneutralizing antibodies to the virion surface antigens that enhance access of the virion-antibody complex to FcγR-bearing cells. Vaccines will need to provide long-term protection against each of the four DENV serotypes by inducing neutralizing antibodies, and live, attenuated and various nonliving virus vaccines are in development.
Here is Paul Offit explaining how dengue vaccines cause harm (at around 11:53):
So you have the neutralizing antibodies and you have the binding antibodies. You want to make sure that the quantity of the neutralizing antibodies that you have, and the persistence of those antibodies, is much greater than the binding antibodies. Because the binding antibodies could be dangerous and cause something called antibody-dependent enhancement.
And we’ve seen that. We saw that with the dengue vaccine…. The dengue vaccine, in children who’ve never been exposed to dengue before, actually made them worse when they were then exposed to the natural virus. Much worse. Causing something called dengue hemorrhagic shock syndrome. Children died because vaccinated children who were less than 9 years of age who had never been exposed to dengue before were more likely to die if they’d been vaccinated than if they hadn’t been vaccinated…. And that was because of antibody-dependent enhancement. (emphasis mine)
Because what happens is, those binding antibodies, they don’t neutralize the virus, they just bind to it. Now we have on our cells something called an Fc receptor, which then can allow the antibody, will bind the antibody and bring the virus into the cell. It’s actually a more efficient way for the virus to enter the cell than otherwise. So what you’re doing by creating all these antibodies is potentially causing this antibody-dependent enhancement which could potentially worsen the problem if you then were exposed to wild-type or natural virus.
This shouldn’t have surprised any informed scientist.
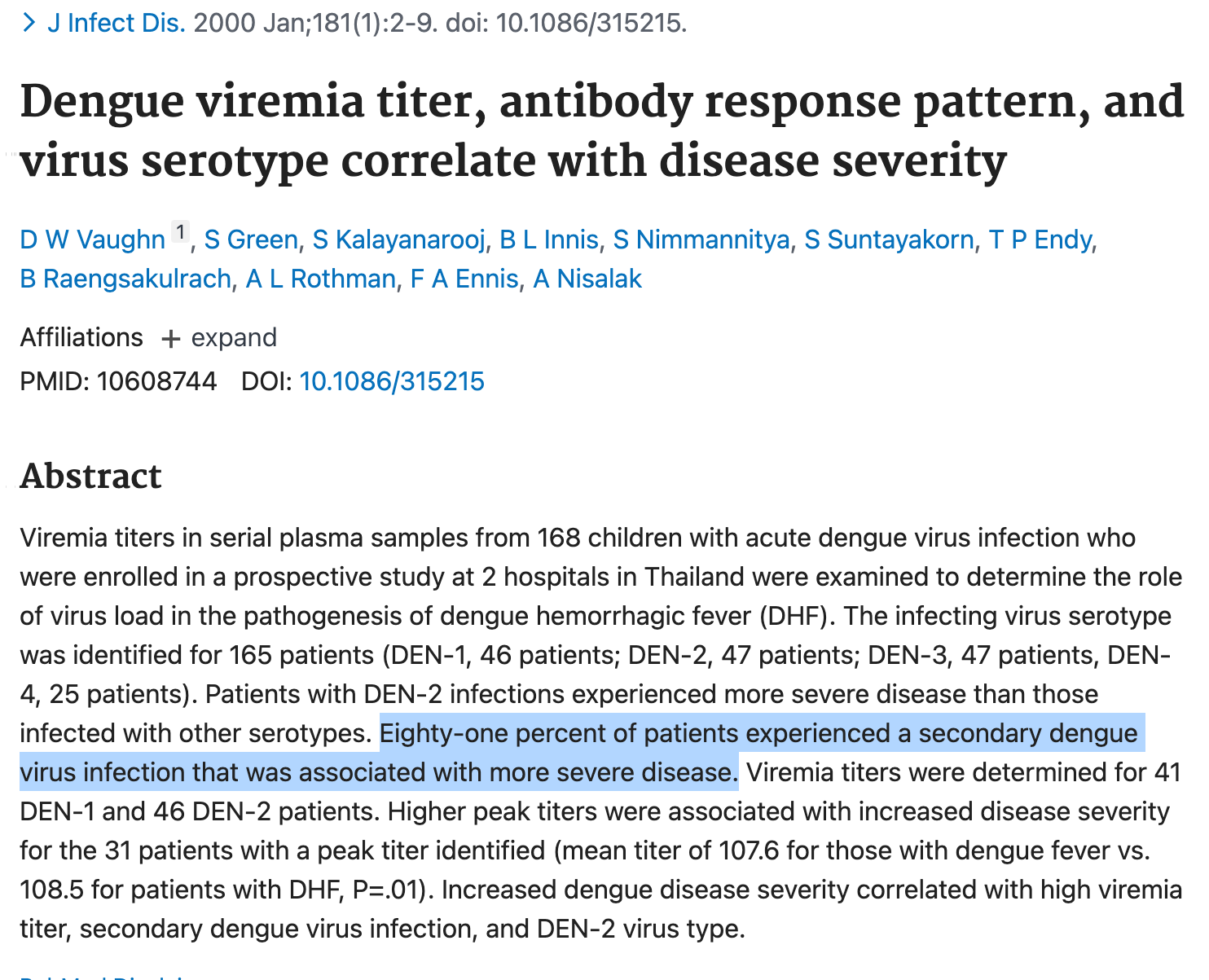
Many studies over many years demonstrated to the scientific community that this would happen. They knew. This 2000 study was among many that demonstrated that “secondary dengue virus infection was associated with more severe disease.”
And if previous studies didn’t drive the point home, Dengvaxia’s own package insert provided plenty of its own clues. Here’s another one that may help explain why dengue has only gotten worse in endemic areas despite an available vaccine:

“Vaccine viremia was observed 7 to 14 days after DENGVAXIA vaccination with a duration of <7 days.”
What happens when uninfected mosquitos bite the recently vaccinated? Has anyone explore this?
As a rule of thumb, public health authorities just wait until we’re scared enough of one risk to accept another. (And we generally have zero understanding of the risks we’re walking into.) Risk hyperawareness is a primer. This hypervigilance is also essentially a prerequisite for autoimmunity.
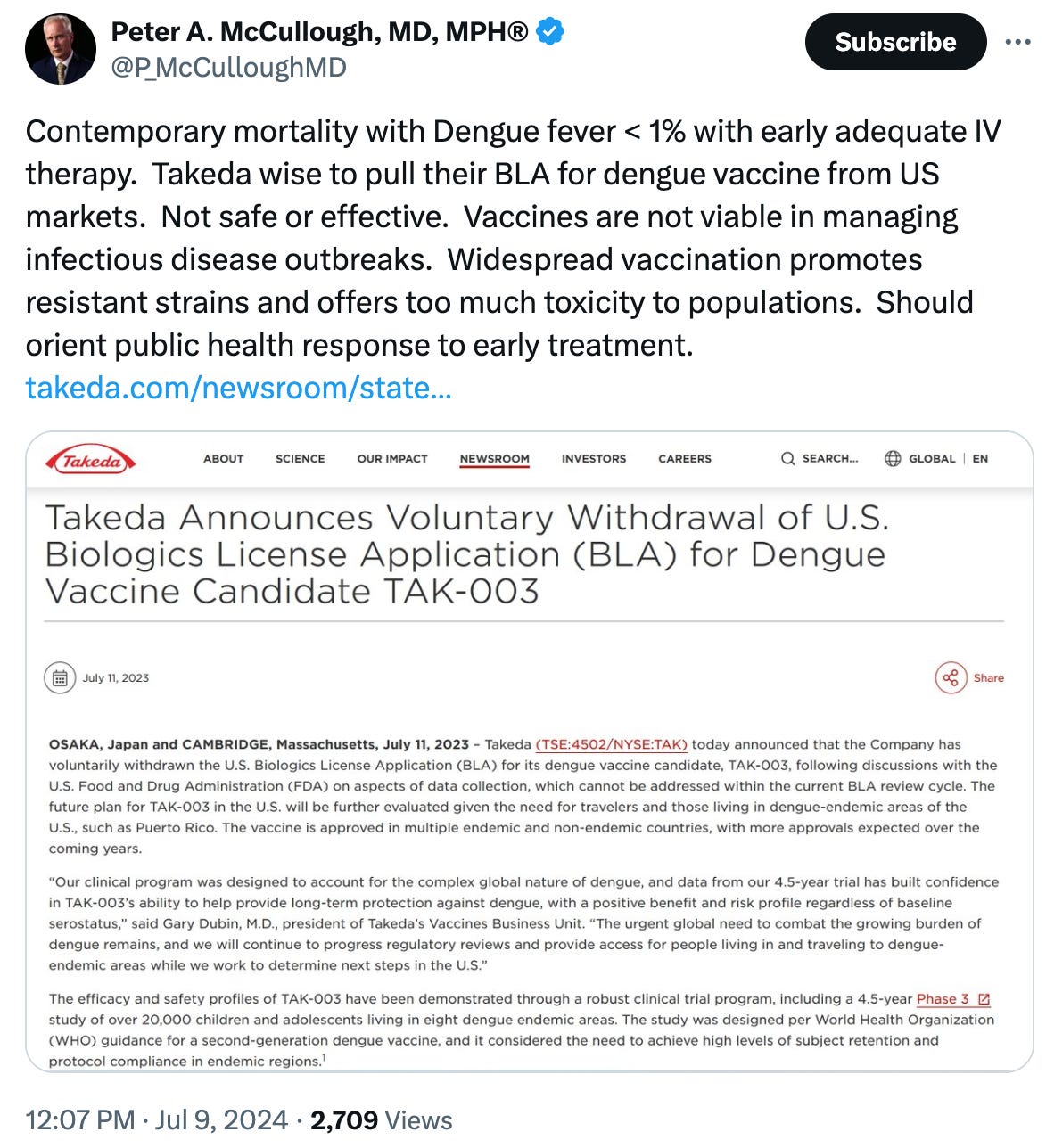
Since the Dengvaxia fiasco, regulators have temporarily backed off, but justifying the need for vaccines is a public health specialty. And there’s also a new tetravalent dengue vaccine on the scene. Takeda’s TAK-003 is based on a live, attenuated DENV-2 virus backbone expressing E and prM proteins of all four DENV serotypes.
Interestingly, Takeda withdrew its U.S. Biologics License Application (BLA) for TAK-003 last year. Dr. Peter McCullough has some thoughts on that…
And then, of course, there are the attempts to turn mosquitos into flying vaccinators.

Keep an eye out for narratives that seek to justify the use of these measures.
Healing Alternatives
If you want to know how the CDC recommends handling dengue cases, you can read the CDC’s Dengue Case Management pocket guide here. It is always helpful to know what your doctors are being told.
But, back in the land of hope and sanity, there are other measures worth exploring.
Below are some other articles referencing natural remedies that your doctor is less likely to hear about:
To date, 31 different species have been found to have the potential to treat dengue; some of these have not yet been investigated scientifically (as indicated in Table 1). In the Philippines, Euphorbia hirta, known locally as “tawa–tawa”, is used in folk medicine to cure dengue fever by people in rural areas [53]. Practitioners of traditional medicines believe that decoction of tawa–tawa leaves can reverse viral infection and prevent the fever from moving into critical stages, although there are no scientific studies proving its effectiveness [54]. Sometimes, tawa–tawa is prepared together with papaya leaves since papaya leaf extract has a function as an antibiotic to cure fever. While papaya leaf extract kills the bacterial infection that caused the fever, tawa–tawa extract prevents bleeding. In addition, unpublished research has found that Psidium guava leaves are a good way to increase platelets, thus helping to avoid bleeding [55]. A water decoction of guava leaves contains quercetin, which acts to inhibit the formation of enzyme mRNA in the virus [56].
This paper also explores medicinal plants and their phytochemicals in inhibiting DENV and SARS-CoV infections.
And here are some remedies you may have some easy access to…
As the headlines come in, let’s approach dengue and each new viral scare from a more informed and empowered place.
Additional reading:


Why is Bill Gates allowed to invest in vaccines after all the deaths and injuries that have occurred and he is being taken to Court for murder and all those children that died and got injured from their experimental vaccines
The elites obviously hate us so much that they’re not happy with eradicating us, but they want to inflict as much disease and destruction before they ultimately do us in…