


Denver Health Administers 1st Shots of an Ebola Vaccine (that sheds)
let's explore why that matters

Ebola is making its rounds through the headlines. This isn’t the first time and it won’t be the last, so let’s pay attention.
This one is troubling.

In a milestone moment in the Mile High City, on Nov. 27, Denver Health administered the first live Ebola vaccine for preventative measures to some patients, 9News reported.
In 2015, HHS designated Denver Health one of 13 Regional Emerging Special Pathogens Treatment Centers in the U.S. — serving as an infectious disease training and care hub for six states in its region.
It is one of the first health systems in the country to administer the vaccine, according to the news outlet.
Does a “live Ebola vaccine for preventative measures” sound like a good idea?
The first question that comes to my mind is, Does it shed?
Turns out it does. From the manufacturer insert (which is a legal document):
“Transmission of vaccine virus is a theoretical possibility. Vaccine virus RNA has been detected in blood, saliva and urine for up to 14 days after vaccinataion. The duration of shedding is not known…”


So, not only does Ervebo NOT stop transmission. It likely contributes to transmission. And it’s being rolled out at “an infectious disease training and care hub for six states in its region.”
Interestingly, the approval of Ervebo was supported by a study conducted in Guinea during the 2014-2016 outbreak that resulted in more than 28,000 cases and more than 11,000 deaths. By far the worst outbreak in reported history. Given that Ervebo is a live virus vaccine that sheds, is it possible that the vaccination study contributed to the outbreak?
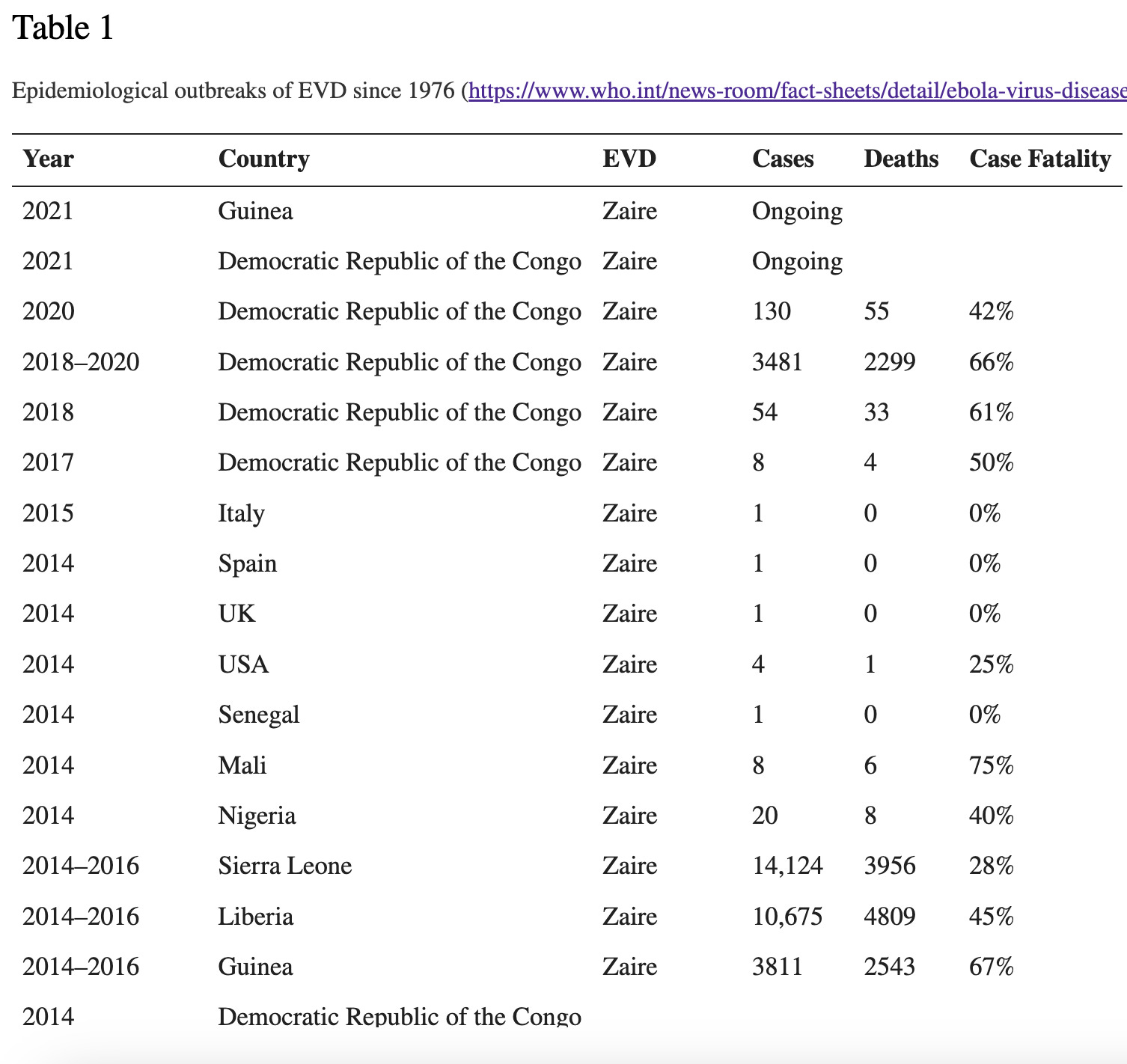
I can’t answer that question, but when I looked up the only other documented outbreak with numbers in the thousands - the 2018-2020 outbreak in the Democratic Republic of Congo (3481 cases and 2299 deaths) - it overlaps with another ebola vaccine study, initiated on May 21, 2018.
Following the April 2018 reemergence of Ebola in a rural region of the Democratic Republic of the Congo (DRC), the virus spread to an urban center by early May. Within 2 wk of the first case confirmation, a vaccination campaign was initiated in which 3,017 doses were administered to contacts of cases and frontline healthcare workers.
https://www.pnas.org/doi/10.1073/pnas.1817329116
(Incidentally, Remdesivir was tested as a potential therapeutic for EBV amidst the 2018-2020 outbreak and demonstrated its ability be more deadly that navigating the virus without treatment.)
We should keep an eye on Denver and anywhere those shots are going into arms…
Back to the package insert…
Vaccine virus RNA was detected by RT-PCR in the plasma of most participants from Day 1 to Day 7 postvaccination with one participant having a positive plasma RT-PCR result 14 days after vaccination.
In other words, viremia.
Regarding the immune response elicited by ERVEBO, we’re also told:
The relative contributions of innate, humoral and cell-mediated immunity to protection from Zaire ebolavirus are unknown.
Under 5.2 Limitations of Vaccine Effectiveness, it states:
Vaccination with ERVEBO may not protect all individuals. Vaccinated individuals should continue to adhere to infection control practices to prevent Zaire ebolavirus infection and transmission.
So… get vaccinated, but don’t assume that you’re protected or that you can’t transmit to others. Sound familiar?
Also, consider the cost of the so-called “protection”:
Decreases in Lymphocytes and Neutrophils White blood cell counts were assessed in 697 participants who received ERVEBO. Decreases in lymphocytes were reported in up to 85% of participants and decreases in neutrophils were reported in up to 43% of participants.
White blood cells play a pretty important role in fighting infections…
And then there are the adverse events, which include fever, sweating, arthralgia, headache, vomiting, diarrhea, rash and parasthesia.
As will all vaccines, ERVEBO has not been evaluated for the potential to cause carcinogenicity and genotoxicity.
Notably, the WHO prequalified the ebola vaccine and the FDA granted Breakthrough Therapy designation for Ervebo, completing its evaluation of the safety and effectiveness of Ervebo in less than six months. Can you say “warp speed”?
Due to the urgent public health need for a prequalified Ebola vaccine, WHO accelerated prequalification by reviewing safety and efficacy data as the information became available. Representatives from the prequalification team participated in the EMA evaluation process to address programmatic suitability for at-risk countries in Africa.
"The development, study, and rapid prequalification of this vaccine show what the global community can do when we prioritize the health needs of vulnerable people,” said Dr Tedros. https://www.who.int/news/item/12-11-2019-who-prequalifies-ebola-vaccine-paving-the-way-for-its-use-in-high-risk-countries
About Ebola
According to the CDC, “Ebola disease is caused by an infection with one of a group of viruses, known as ebolaviruses, that are found primarily in sub-Saharan Africa. Although *Ebola disease is rare, people can get the disease through contact with an infected animal (bat or nonhuman primate) or a sick or dead person infected with an ebolavirus.” *emphasis mine
Six species of Ebolavirus have been identified: Zaire, Bundibugyo, Sudan, Taï Forest, Reston and Bombali. (The vaccine was only designed to address Zaire.)
EVD has an incubation period that ranges from 2 to 21 days. Onset of symptoms of ebolavirus disease can include fever, fatigue, myalgia, headache and sore throat. More serious and advanced cases can include vomiting, diarrhea, rash, impaired kidney and liver function and in some cases internal and external bleeding. Caregivers, including health care workers who do not use correct infection control precautions, are at the highest risk for infection.
Case fatality rates have varied from 25–90% in past outbreaks, depending on circumstances and the response. Clearly circumstances and response play a significant role.
Treatment strategies for infected patients include hydration, replacement of electrolytes, nutritional support, maintaining oxygen status and blood pressure and treating other infections.
In case you were wondering, nature offers some measures for managing the symptoms of ebola. (Not giving medical advice - just passing along what I’ve found)
This site recommends home remedies like garlic, green tea, elderberry, probiotics, olive leaf extract, vitamin C, selenium and tumeric. This site seconds some of those recommendations.
Let’s hope we never have to put any of these measures to the test. But considering the potential for these shots to start an outbreak here at home, maybe it’s time to stock up.
These are definitely not vaccines. I believe from this point forward, nobody should get any type of “medicine” injected into them. Well, unless you wanna die, then by all means, go ahead.
Colorado has always been such an ebola hotspot. Better safe than sorry.