


Expert testimony exposes widespread medical negligence within the pediatric health care system and Robert Roberson's judge needs to hear it.

What I know is that these children’s mismanaged medications, because of the lack of an expert that knows everything about having pediatric pharmacology on their team, is causing a massive disservice to these children.
- Dr. Jena Quinn, PharmD, BCPPS
In her recent testimony before the Assembly Health Committee last week, Jena Quinn, a pediatric pharmacist, exposed rampant pediatric medication errors linked to systemic lack of education and oversight.
Her testimony was in support of NJ A4810, a bill that would require NJ FamilyCare reimbursement for pediatric medication management services provided for certain children by licensed pharmacist.
According to Quinn:
1 in 3 pediatric prescriptions contain an error.
Less than 1% of pharmacists are trained to address the unique needs of pediatric patient.
Pharmacists in retail settings are not required to have any education in pediatrics.
Pediatricians do not oversee a patient’s medications once they have referred them out to a subspecialist.
A study that introduced the intervention of pediatric pharmacists demonstrated a 44% reduction in hospitalizations in children with medical complexities.
You can listen to her complete testimony here (at about 32:00)
Hi my name is Jena Quinn. I am a pediatric pharmacist. A lot of people don’t even know what that means. So a pediatric pharmacist is a pharmacist that has gone to school to get their doctorate of pharmacy, but then after we practice, we get our residency just like a normal residency doctor training for 1-2 years. After that we go on to get our board certification in pediatric pharmacology. So our training is very unique and it’s very, very intensive. There’s only 1700 of us in the United States…
I’ve been a pediatric pharmacist for over a decade. I practice at the Children’s Hospital of Philadelphia as well as Cooper University. I’m coming to you today not only as a business owner of Perfecting Peds, I’m coming to you today as a pediatric pharmacist.
There’s a massive problem that is under recognized in the United States. One in 3 pediatric prescriptions contain and error. The USP Medication Error Report of 2023 showed that 31% of pediatric prescriptions contain an error. I can tell you as a mom of 3 little girls that I have intervened on 60-70% of my own daughters’ medications. This being said, 85% of medications in the pediatric population are off-label. Pediatricians only have 1-2 semesters of pharmacology. Because of that, they are really great at their core medications – 20-30 meds. But as they start to branch out and the patient gets more complex, and they start referring out to subspecialists, what happens is that pediatricians have a very hands off approach.
I’ve been told by an innumerable amount of pediatricians that once a subspecialist takes over, they will not touch their medications. What not a lot of people are aware of in the United States is that pharmacists in the retail setting are not mandated in school to have any sort of pediatric education. There’s a small subset of us that have elected to take a pediatric elective during school. That means less than 1% of us are trained to take care of children and are trained to know all the ins and outs of the unique pharmacology, kinetics, weight adjustments that a pediatric patient needs. Because of this, the retail pharmacist in the United States does not even have access to the child’s weight. That is how we dose medications for children. And this is why 1 in 3 children are inflicted with a medication error in 2023.
We have this unique skill set of pediatric pharmacists who, until the birth of my business (and I’m not saying this to solicit my business, I’m coming to you as a mom and a pediatric pharmacist), we’ve been contained in the hospital walls. So if you ever come across a pediatric pharmacist it will be in the hospital when your child is acutely ill. We have this unique skill set and we are one of the only medical professionals that can flex across all meds.
I’m going to share this with you again as a pediatric pharmacist… I went to local medical daycares, subacute rehabs as well as long-term care facilities in the New Jersey area. I was able to pilot what is now Perfecting Peds in 400 of our kids in NJ. I was able to publish my findings, our findings as a group, of what happens when you put a pediatric trained pharmacist in the care of children with medical complexities in the ambulatory care setting. So what happens… just like a pediatrician, you have a pediatric pharmacist seeing these children upwards of 12x/year, a minimum of 4x/year. What we found was what I knew what would happen, but astounding. We were able to show a 44% reduction of hospitalizations. So from year 0 to year 1… we were able to decrease hospitalization almost by half. We identified 13 ways in our first 102 kids - interventions of how we can optimize therapy, but always ways that we can negate major medication errors. We were also able to show in direct cost that, although polypharmacy is something only talked about in the geriatric population, it heavily impacts our pediatric population: in epilepsy, in behavioral health, in sickle cell. All of these children do have a lot of medications on their profile and no one owns the question “should we take this medication off? Is it time?”
We were able to de-prescribe 15% of medications and decrease the average burden of medications for these children from 23 to 20 medications. Because of this, we were able to show in our first 102 patients an $11,000 total cost of care savings in each child annually…
What I know is that these children’s mismanaged medications because of the lack of an expert that knows everything about having pediatric pharmacology on their team is causing a massive disservice to these children.
(You can read her published study here.)
Based on what we learn here, A4810 is just another bandaid for an enormous systemic problem. This is subsidizing more experts to oversee the experts we were told to trust in the first place. What does this say about the people we’re told to put our faith in?
The implications of Quinn’s testimony are pretty astounding as they highlight the failure of pediatricians to properly prescribe and monitor the medications they give to children.
Either pediatricians are not properly trained to medicate medically complex children or there’s zero oversight of the care of these children. Or both.
This is concerning.
The Curious Case of Robert Roberson
This testimony was particularly striking because it occurred last Thursday, on the same day Robert Roberson was scheduled to be executed for the death of his daughter, which was attributed to “shaken baby syndrome.”
In this story, we say the medical consensus today is that the diagnosis of ‘Shaken Baby Syndrome’ (SBS) in criminal cases is based on “junk science.” There is growing skepticism of SBS and fierce debate within the medical community and in the courts, several of which have ruled the diagnosis is discredited and overturned SBS convictions. A New Jersey appeals court ruled that it’s based on “junk science.” But other courts and the American Academy of Pediatrics dispute that characterization and uphold the clinical and medical validity of SBS.

“More than a decade ago, the Texas Legislature passed Senate Bill 344, which allowed challenges to convictions that were based on disproven or incomplete science,” read a letter from 86 bipartisan House members. “That law passed with unanimous support of the Texas House because we recognized that innocent people are sometimes wrongfully convicted based on scientific evidence that later turns out to be wrong.”
Perhaps the judge should hear Quinn’s testimony, given the other details of this case…
From A Midwestern Doctor:
Many existing medical conditions could have explained his daughter’s death (e.g., in the 5 days before her death, she had continual vomiting, coughing, and diarrhea). Likewise, when she was seen at the ER for this, her doctor inappropriately prescribed two drugs (which now have warnings for being given to children due to the drugs causing breathing difficulties and death) then shortly after went to sleep, stopped breathing and died (which the father—who had slept with her in his arms because he was worried about her—noticed when he woke up next to her and she had turned blue). Likewise, she had many signs of pneumonia and sepsis that numerous medical experts have since testified were the actual cause of her death. Sadly however, her ER doctor did not recognize this and instead simply gave her an opioid to reduce her symptoms, which was at lethal levels in her blood at the time she died (likely triggering respiratory arrest—and now has a blackbox warning against giving it to children for this very reason) along with an anti-nausea drug which was also found at dangerously high levels and no longer given to children because it can cause respiratory arrest.

Roberson had been set to become the first person in the U.S. executed over a murder conviction connected to a diagnosis of shaken baby syndrome. He was taken to America's busiest death chamber last Thursday but a last-ditch effort by lawmakers to buy Roberson more time stopped his execution at the eleventh hour… (emphasis mine)
Roberson's claims of innocence are backed by a group of Republican and Democratic legislators who say he was convicted based on outdated science…
In a dramatic turn of events, Robert Roberson's execution was stopped just days before it was set to occur, spotlighting Texas' controversial 2013 junk science law. This law allows for relief if the evidence in a conviction is discredited, yet Roberson's case exposes systemic weaknesses.
Convicted in 2002 for the murder of his daughter, his supporters argue that the case was built on outdated and flawed scientific evidence. A coalition of lawmakers, experts, and even the original prosecutor now support him, citing new science debunking shaken baby syndrome.
The impact and interpretation of the law will be scrutinized by a House committee, with Roberson's testimony playing a key role in what many see as a necessary debate over wrongful convictions and judicial reform.
This is a big deal.
Robert Roberson deserves justice. And so does everyone. This case will determine some important precedents regarding “shaken baby syndrome”, “junk science” and the death penalty.
To be clear, BigPharma needs diagnoses like “shaken baby syndrome” and “SIDS.”
This case, in part, determines the fate of the validity of a diagnosis that is essentially gaslight that deflects from medical/pharmaceutical causes that are far more likely. It also determines the fate of some of the most hideously gaslit among us: accused parents of children who may have been killed by medical interventions.
Medical error is very real, particularly with regard to children.

The potential for adverse drug events within paediatric inpatient populations is about three times as high as among adults, and it is estimated that one in four children experiences an adverse drug reaction during hospitalisation. In a recent study investigating serious patient safety events in 44 children’s hospitals, more than 20% of severe accidents were caused by MEs.

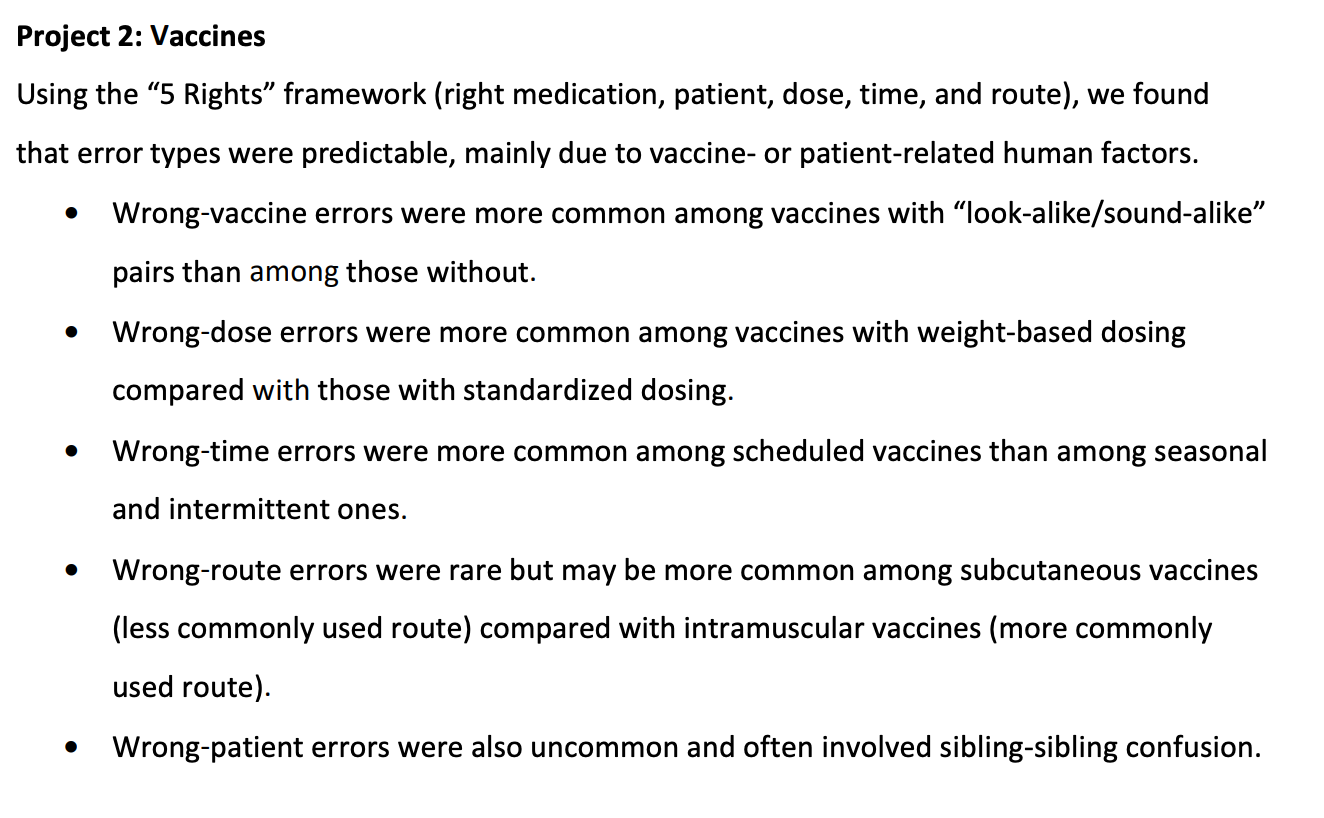
This report included medical errors linked to pediatric vaccines…
Let’s end this nonsense, save Robert’s life and start looking out for children in earnest.
So sad that overdosing, misdosing, confused dosing and over-medicating children has gotten to the point where parents are being tried for murder of their own children when the medical errors are off the charts. As a parent, imagine losing a child, being blamed for that death, and then being tried for murder when it was the doctor’s fault. Doctors simply should not be paid Any sort of fees when they kill children. Doctors also should be required to take pediatric pharmacology and properly dose their patients With oversight because if 1 in 4 are incorrect, that's an astounding amount of inaccuracy, With our own children paying the price., and it just further lessens the public faith in the medical system.
The War On The Child: Battlefront “Pediatricians: The Worst Kind Of Evil”
https://open.substack.com/pub/anntomokorosen/p/expert-testimony-exposes-widespread