A new study has shown that people vaccinated against Ebola who still developed the disease had a substantially lower risk of dying than people who were not vaccinated, even if they received the vaccine when they were already infected with the virus.
It’s almost like they’re hoping we miss the “people vaccinated against Ebola… still developed the disease” part.
In this retrospective cohort analysis of patients with confirmed Ebola virus disease admitted to Ebola health facilities in the Democratic Republic of the Congo between July 27, 2018, and April 27, 2020, we performed univariate and multivariate analyses to assess case fatality risk and cycle threshold for nucleoprotein according to vaccination status, Ebola virus disease-specific treatments (eg, mAb114 and REGN-EB3), and other risk factors. (emphasis mine… and remember this)
We analysed all 2279 patients with confirmed Ebola virus disease. Of these 2279 patients, 1300 (57%) were female and 979 (43%) were male. Vaccination significantly lowered case fatality risk (vaccinated: 25% [106/423] vs not vaccinated: 56% [570/1015]; p<0·0001). In adjusted analyses, vaccination significantly lowered the risk of death compared with no vaccination, with protection increasing as time elapsed from vaccination to symptom onset (vaccinated ≤2 days before onset: 27% [27/99], adjusted relative risk 0·56 [95% CI 0·36–0·82, p=0·0046]; 3–9 days before onset: 20% [28/139], 0·44 [0·29–0·65, p=0·0001]; ≥10 days before onset: 18% [12/68], 0·40 [0·21–0·69; p=0·0022]; vaccination date unknown: 33% [39/117], 0·69 [0·48–0·96; p=0·0341]; and vaccination status unknown: 52% [441/841], 0·80 [0·70–0·91, p=0·0011]).
I don’t have access to the full study, but the summary doesn’t account for disease-specific treatments used or other risk factors other than “Longer time from symptom onset to admission significantly increased risk of death (49% [1117/2279], 1·03 [1·02–1·05; p<0·0001]).”
Fauci Fingerprints?
Importantly, another (NIAID-funded) clinical trial was also taking place during the same outbreak:
From November 20, 2018, to August 9, 2019, a total of 681 patients were enrolled and underwent randomization at Ebola treatment centers in Beni (335 patients), Butembo (243 patients), Katwa (46 patients), and Mangina (57 patients)…
Presumably, a “retrospective cohort analysis of patients with confirmed Ebola virus disease admitted to Ebola health facilities” during this time would have included these people…
Patients were assigned in a 1:1:1:1 ratio to receive ZMapp (a triple monoclonal antibody agent), remdesivir (a nucleotide analogue RNA polymerase inhibitor6), MAb114 (a single human monoclonal antibody derived from an Ebola survivor7,8), or REGN-EB3 (a coformulated mixture of three human IgG1 monoclonal antibodies9,10).
The trial was jointly approved by the ethics board at the University of Kinshasa and the institutional review board at the National Institute of Allergy and Infectious Diseases (NIAID) and was overseen by an independent data and safety monitoring board. *emphasis mine
A total of 673 patients were included in the primary analyses. At 28 days, death had occurred in 290 patients (43.1%) overall
And does this finding from the 2019 study sound familiar?..
The percentage of patients who died was lower among those who reported that they had received the rVSV∆G-ZEBOV-GP vaccine than among those who reported no vaccination (27.1% [42 of 155 patients] vs. 48.4% [225 of 465]). However, patients who reported vaccination were also more likely to have had fewer days of illness before enrollment, higher baseline nucleoprotein Ct values, and lower levels of alanine aminotransferase (Table S5).
Is it me, or does this seem like the preface for the “new study”?
The study seems designed to find a favorable outcome for the vaccinated. And yet fewer deaths from Ebola was the best they could do. Yikes.
That’s concerning, as we’ve already started giving it to health care workers in the states.
Does a “live Ebola vaccine for preventative measures” sound like a good idea?
The first question that comes to my mind is, Does it shed?
Turns out it does. From the manufacturer insert (which is a legal document):
“Transmission of vaccine virus is a theoretical possibility. Vaccine virus RNA has been detected in blood, saliva and urine for up to 14 days after vaccination. The duration of shedding is not known…”
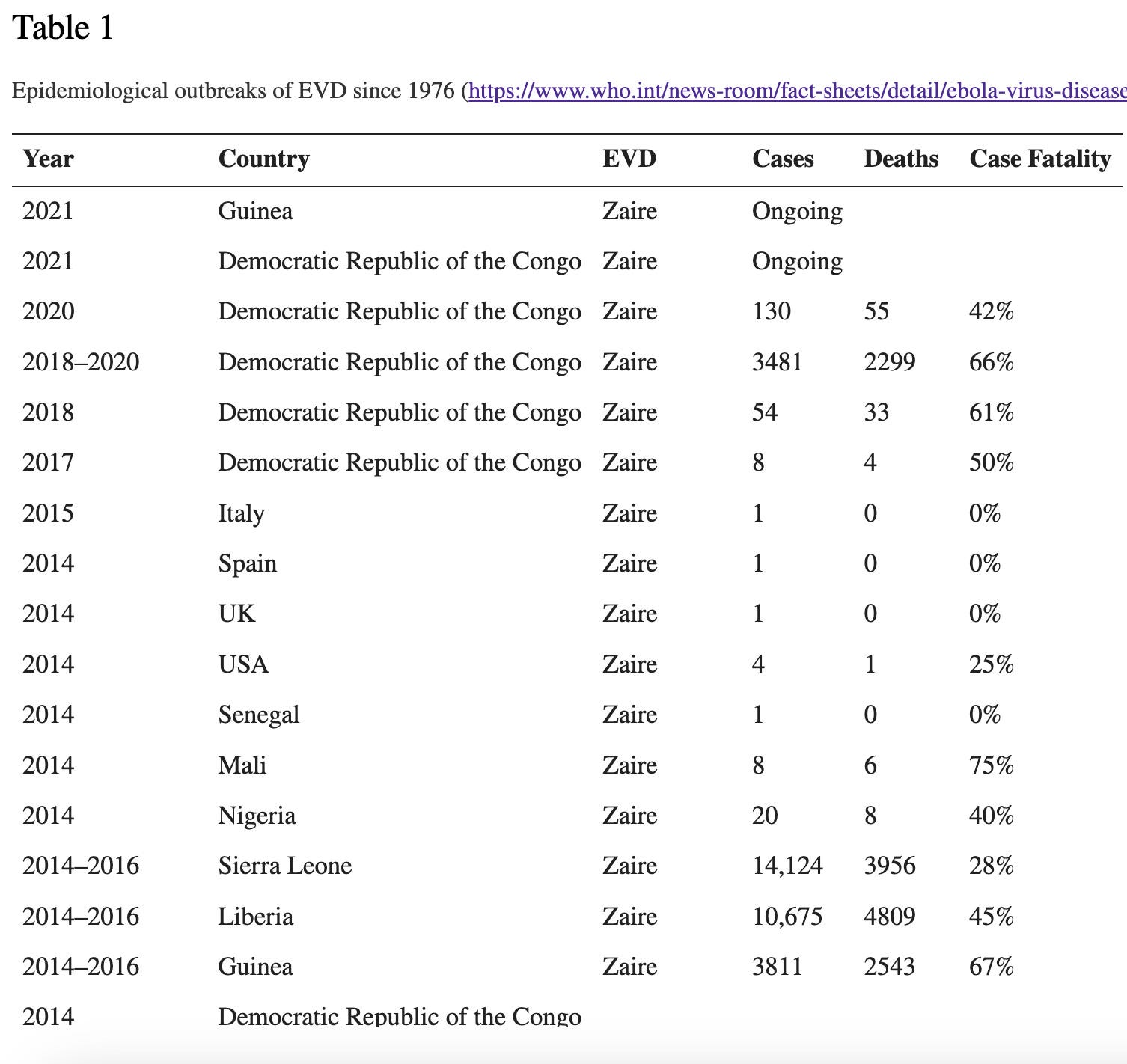
Interestingly, the approval of Ervebo was supported by a study conducted in Guinea during the 2014-2016 outbreak that resulted in more than 28,000 cases and more than 11,000 deaths. By far the worst outbreak in reported history. Given that Ervebo is a live virus vaccine that sheds, is it possible that the vaccination study contributed to the outbreak?
I can’t answer that question, but when I looked up the only other documented outbreak with numbers in the thousands - the 2018-2020 outbreak in the Democratic Republic of Congo (3481 cases and 2299 deaths) - it overlaps with another ebola vaccine study, initiated on May 21, 2018.
Following the April 2018 reemergence of Ebola in a rural region of the Democratic Republic of the Congo (DRC), the virus spread to an urban center by early May. Within 2 wk of the first case confirmation, a vaccination campaign was initiated in which 3,017 doses were administered to contacts of cases and frontline healthcare workers.
I find this interesting. Because the numbers are there for any researcher who wanted to explore them: 3481 cases and 2299 deaths (see chart above). A vaccine clinical trial was taking place during this outbreak during which 3,107 doses were administered. Why not return to the records that produced these numbers and cross-reference vaccination status from records that should have been kept in clinical trials? Why instead a retrospective cohort analysis of patients with confirmed Ebola virus disease admitted to Ebola health facilities where experimental treatments were also being administered?
Consider ALL of these things and think about how much time, money and manipulation goes into the creation of the headlines we read. Remember this when you read ANY headline.